
Diphtheria: A look into disease breeding grounds in the wake of diphtheria outbreak in Kano

The Nigeria Centre for Disease Control (NCDC) has declared an outbreak of diphtheria on 20 January 2023, the worst in a decade. The outbreak was first notified in Kano and Lagos states on 1 December 2022. In this report, Arinze Chijioke looks at the factors contributing to the outbreak in Kano, the epicentre of the outbreak.
This April, 7-year-old Musab Kabir started having a runny nose, fever, constant headaches and sore throat. He complained to his father, Kabir who quickly rushed to the Mongoro Primary Healthcare Centre (PHC) in Tudun Fulani Barebari, his community in Ungogo local government, Kano State.
“At the hospital, they did not carry out any test but gave us some medication and said it will help to calm him down, they asked us to go home,” said Kabir.
Back home, the situation became worse and Kabiru took his son to the Murtala Muhammad Specialist Hospital (MMSH) where they were admitted for 3 days. At the MMSH, a Diphtheria test was undertaken and it came out positive.
Afterwards, Diphtheria antitoxin (DAT) was administered to him to stop the bacteria toxin from further damaging his body after which antibiotics were given to eliminate the bacteria and prevent further transmission to others.

Read Also: Bandits’attacks on health facilities in Kaduna leave residents without access to healthcare
The Deadly Infection
Diphtheria is a bacterial infection which is transmitted through respiratory secretions, or by breathing in droplets from an infected person when they cough or sneeze. The symptoms include fever, runny nose, sore throat, cough, and neck swelling amongst others.
In severe cases, a thick grey or white patch appears on the tonsils and/or at the back of the throat associated with difficulty breathing, according to the NCDC.
In an interview with Africa Check, Dr Adeboye Muhammed, an associate professor of paediatrics and child health at the University of Ilorin said that most infections do not show symptoms or are mild. For those that do, symptoms usually start two to five days after someone becomes infected.
Diphtheria can be passed from one person to another through close contact, respiratory droplets, or contaminated items. The disease can be fatal, but treatment with antibiotics and antitoxins can save lives.
“If the toxin gets into the bloodstream, it can cause heart, nerve, and kidney damage. Where the disease is coupled with poor hygiene, infection of the skin is also common, leading to pus-filled blisters, including on the legs and hands,” a report by the US Centre for Disease Control and Prevention (CDC) shows.
Kano at the centre of the outbreak
As Musab was being attended to, his father returned home to discover that his 4-year-old sister, Fatima was displaying the same symptoms. Sadly, he could not take her to the Murtala Muhammad Specialist Hospital , MMSH for treatment because it was late and the hospital was quite far from his community.
To make matters worse, the primary healthcare centre in his community lacked the capacity to treat Diphtheria. And so, he decided to wait till the next morning to take her to the hospital for treatment. But she died that night.
“My daughter would not have died if our community health centre could handle the disease, “Kabir regretted. “There was no way we could get medication for her the night she died.”
Fatima was one of many children who have died following the outbreak of diphtheria in Kano State. The lack of access to healthcare in remote and underserved areas has made it difficult to detect and treat diphtheria cases early, which has led to further transmission and more deaths.
As of January 2023, the Kano State Ministry of Health confirmed that 25 persons- mostly children had been killed following the outbreak which was reported to have begun in Bare Bari community, Ungogo local government area (LGA) where at least 11 people were reported dead.
Out of a total of confirmed 389 cases across 21 states as of March 15, Kano State alone had 377 cases, translating to 44.7% and 56 deaths out of 62 recorded nationwide, according to a situational report from the National Centre for Disease Control (NCDC).
Since the outbreak of the disease in Kano, only Aminu Kano Teaching Hospital, (AKTH) and the Murtala Muhammad Specialist Hospital, (MMSH) are the facilities with the capacity to manage victims. The NCDC established two isolation wards with a capacity of 80 beds at the MMSH with support from Doctors Without Borders (MSF) and the state health ministry.
While communities such as Tudun Fulanin Barebari have existing health facilities, they lack the capacity to treat epidemics such as Diphtheria. In other communities visited, there is a complete lack of healthcare facilities.
Research on Epidemic Preparedness: Funding Health and Disease Control by Budgit, an innovative enterprise passionate about simplifying the Nigerian budget found that the doctor density in Kano is worrying with fewer than 1 doctor per 10,000 persons which is way below the Sustainable Development Goal (SDG) of 44.5 doctors, nurses and midwives per 10,000.
Read Also: After SOLACEBASE report, Jigawa govt distributes palliatives to flood victims from donated fund
In an interview with SOLACEBASE, Kano state Epidemiologist, Dr. Abdullahi Kauranmata said that Diphtheria is not just managed anyhow and anywhere but at designated isolation centres which are usually limited in number to ensure that other facilities are able to continue to provide routine services and so that the patients don’t get mix up the with others.
“When we saw that the numbers were beginning to rise, we planned to scale up the centres, we already have satellite centres that we could activate and that will be managed according to the protocol, “he said.
He however explained that clinicians are sensitized and trained to raise suspicion where necessary and refer directly to the two existing centres where they access care.
Squalid living conditions contribute to the outbreak
Among those who are most at risk of contracting diphtheria, according to the NCDC are people who live in a crowded environment and those who live in areas with poor sanitation.
Across much of the rural communities in Kano state, a haunting neglect of sanitation and sanitation facilities prevails. The site of soak-away pits and gutters overflowing with dirty water around residential areas is common. Children are often seen playing around this environment.
It is also common to see both adults and children squatting and defecating into trenches and pools of floodwater water.
In 2021, the state government declared a state of emergency on Water, Sanitation and Hygiene (WASH) so as to end open defecation. It pledged to provide mobile toilets and more public conveniences in the state. Regrettably, these commitments have not materialised as anticipated.
Read Also: Stakeholders advocate 70 per cent of health budgetary allocation for PHC
The community head of Gwagwarwa in Nassarawa local government, Abdulhamid Muhammed said that the declaration was a sham as some residents of his community and other locations still practice open defecation.

In Nassarawa and Ungogo, access to safe drinking water is a challenge. As a result, residents often rely on water vendors, locally known as Mai Ruwa, to get water. However, some of these vendors get water from sources that are close to dirty environments. For instance, the jerrycans used to store water by the vendors often go months without proper cleaning. This can lead to the spread of germs and bacteria, which can cause serious health problems, such as diarrhoea, cholera, and typhoid fever.

Moreover, residents often pay no attention to the unsanitary state of the surroundings where the water is gotten.
“Because of the scarcity, we just want water and don’t care where it is coming from,” he said. “We believe that provided it is borehole water, it is drinkable,”. “Oftentimes, if their pipe falls inside dirty water or on the ground, they pick it up without washing it and continue to fetch, “said Muhammed.

Inadequate vaccine delivery at the heart of the outbreak
As the first dose of the vaccine was administered across the five epicentres of the outbreak in Kano. Ado Isah made sure that his children were vaccinated.
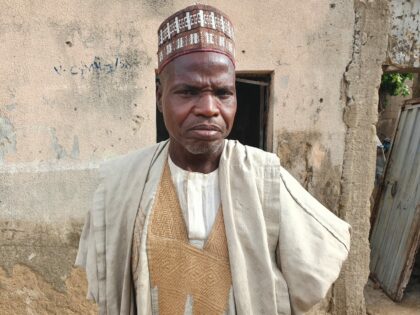
Yet, Muhidden, one of his sons, was infected with the virus. Isah, who is the community head of Tudun Fulani Barebari said that he became confused after he found out that his child had Diphtheria even after he was vaccinated.
“I had to take him to the Murtala Muhammad Hospital where he was admitted for four days and given the necessary treatment before he was discharged,” Muhidden said.
He said that as the leader of his community, he has made efforts to ensure that the outbreak is curtailed by sensitizing residents on the need to always keep their surroundings clean. He also said that while the government has made some efforts, following the outbreak, the inadequacy of vaccines remains a challenge, adding that some parents are having to depend on traditional herbs such as moringa powder, baobab and hibiscus leaves for the treatment of the outbreak which is not effective.
Read Also: Investigation: How Rep member, agency abandoned communities, siphoned project funds in Benue State
The Nigeria childhood immunisation schedule recommends three (3) doses of pentavalent vaccine (diphtheria toxoid-containing vaccine) which protects against 5 life-threatening diseases – Diphtheria, Pertussis, Tetanus, Hepatitis B and Hib – in children in the 6th-, 10th- and 14th -week of life.
However, inadequate vaccination coverage has been identified as another major driver of the outbreak in Kano. The state’s child vaccination rates are well below both the national average and the target/world average.
At a webinar organised by the NCDC in March, the Head of the emergency paediatric unit at the Murtala Mohammed Specialist Hospital in Kano, Salma Ali Suwaid said that only 20 per cent of children aged four to 14 were fully vaccinated with tetanus and diphtheria vaccines in the state. She said that ten per cent were partially vaccinated and 54 per cent were not vaccinated.
Former Commissioner for Health in the state, Dr. Aminu Ibrahim Tsanyawa said that the low routine immunization which is responsible for the spread of the disease is due to the hard-to-be-reach areas in the state.
In a statement to SOLACEBASE, Director General of the NCDC, Dr Ifedayo Adetifa said that Historical sub-optimal vaccination coverage is the main driver of the outbreak given the most affected age group (2-14-year-olds) observed and a national survey of diphtheria immunity that found less than half (41.7%) of children under 15 years old are fully protected from diphtheria.
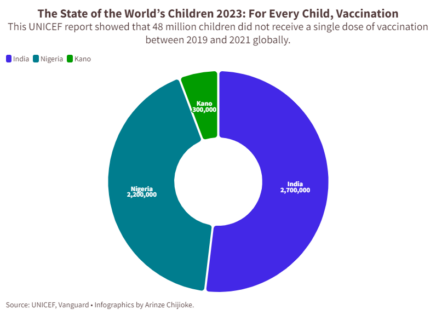
In its report, the State of the World’s Children 2023: For Every Child, Vaccination released in April, the United Nations International Children’s Emergency Fund, (UNICEF) found that Nigeria alone- second only to India- had 2.2 million unvaccinated children between 2019 and 2021. Out of this number, an estimated 300,000 children were unvaccinated in Kano according to UNICEF’s Chief Field Officer in the state, Mr Rahama Farah.
The Director of Disease Control and Immunisation at Nigeria’s National Primary Health Care Development Agency (NPHCDA), Bassey Okposen said that a total of 500,000 doses of Tetanus and diphtheria (Td) vaccines had been supplied to Kano state for the vaccination of age group four to 14 years.
However, speaking on behalf of Okposen at the NCDC webinar, Dr Adejoke Oladele, also of the NPHCDA said that the agency used the Td vaccine stock which was meant for pregnant women because of the scarcity. She said that the agency was still trying to get more into the country to cover the age group above those that are for routine immunisation.
For the adequate medical management of cases, the World Health Organization, WHO recommends that sufficient quantities of diphtheria antitoxin should be available nationally or regionally.
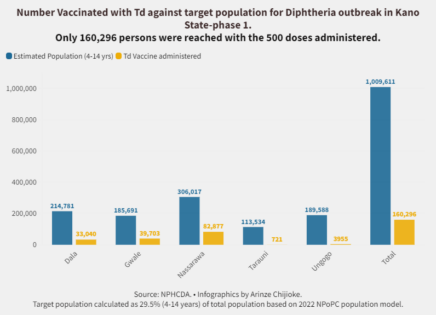
But across Dala, Gwale, Tarauni, Nassarawa and Ungogo- the five local governments which are the epicentres of the outbreak, with an estimated population of 1,009,611, only 160,296 persons were reached with the 500,000 doses administered, according to data from the NPHCDA.
Kano State Primary Health Care immunisation officer, Abdullahi Muhammad claimed that over 270,000 were vaccinated in the first phase and that an additional 350,000 persons were vaccinated in the second phase between March and April, bringing the total to over 620,000.
“We are waiting for the third and final phase of the vaccination, “he said. “We requested 1 million doses, but they gave us 500,000. Our intention is to reach 1.5 million people in the third phase. But we don’t know when the final dose will come.”
Kauranmata said that there is inadequate Td vaccine-the best we can use for mass reactive vaccination to prevent community transmission-because of the regulations and policies that guide its procurement. However, he noted that the federal government and the NPHCDA are working to ensure that there are enough supplies to Kano giving its population.
Muhammad also pointed out that not much awareness was created across communities in the state about the disease, its symptoms, vaccination and its importance for the prevention of further outbreaks of the disease.
When Usman Suleiman complained that he was having fever, headache, running nose, and coughing one evening last May, his mother, Aisha thought her son had malaria.
Aisha, a resident of Gwagwarwa, Nassarawa LGA in Kano, immediately went to a chemist where she bought malaria drugs and gave them to her son. However, the situation worsened, and his jaws began to swell.
Read Also: Diphtheria Outbreak: FG blames poor immunization performance
“I called some of my neighbours, who told me that Suleiman was showing signs of diphtheria. They advised me to take him to P&P Primary Healthcare Centre in Nassarawa immediately. There, he was admitted and given treatment for diphtheria.”
Usman is fully recovered now and the entire family members have received the first dose of vaccination against the disease. The village head of Gwagwarwa, Abdulhamid Muhammed admonished that the government must ensure that there is adequate vaccine delivery as that is the only way to tackle the outbreak.
“There is also the need to equip primary healthcare centres with the right facilities so that patients would not have to always be referred to the Murtala Muhammad Specialist Hospital for treatment when such outbreaks occur,” he said.
Huge allocation, poor releases
Over the years, Kano State has grown its health budget share, especially concerning epidemic preparedness in line with increased prioritization and the need to invest significantly to improve its poor health metrics. Its health budget rose from single-digit figures to double digits and exceeded the 15 per cent mark to which several nations (Nigeria included) committed in the Abuja declaration of 2010 in 2019 and 2020.
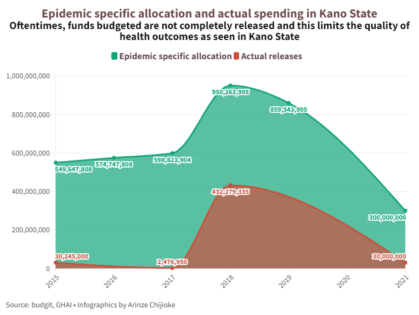
However, findings show that the allocations have often not been completely released and utilised, leading to few results. In 2015, for instance, the state allocated N549,647,808 to epidemic preparedness but released N30,245,000. In 2016, 574,747,808 was allocated but nothing was released. In 2017, N598,823,904 was allocated, but only N2,476,950 was released. Out of N950,263,905 that was allocated in 2018, N432,279,335 was released. In 2019, N859,543,905 was allocated but no amount was released.
In 2020, the state created the Epidemic Preparedness and Response (EPR) budget line for fiscal year 2021, with funding increased by 33 per cent for fiscal year 2022 totalling over N400 million (US $960,000).
Separately, the 44 local government areas (LGAs) in the state also allocated 2 million Naira each to strengthen EPR-related activities, increasing EPR spending by 88 million Naira. This is followed by advocacy by the Legislative Advocacy Initiative for Sustainable Development Goals (LISDEL) and Global Health Advocacy Initiative (GHAI).
Read Also: Investigation : Jigawa residents may be disenfranchised as INEC fails to replace lost PVCs
Out of a total of N300m budgeted for epidemic preparedness in 2021, N30m was approved and released by the state governor, Abdullahi Ganduje on August 2, 2021.
The Budget research also found that untimely and incomplete release of available funds limits the quality of outcomes which relevant agencies can accomplish within the intended fiscal time frame.
In his address during a multisectoral forum on Epidemic Preparedness and Response Financing by LISDEL, Ibrahim, the former health commissioner affirmed that the COVID-19 era has further stressed “the importance of preparedness and health financing for health security.”
Vaccine hesitancy yet remains a challenge
Musa Haruna, a resident of Tudun Fulanin Barebari was aware when the first dose of the Diphtheria vaccine was administered but he stopped his four children from being vaccinated because of his disbelief in the efficacy of vaccines.

“I heard that if a child gets vaccinated, it reduces his life span or results in other unknown illnesses, “he said. “My children are healthy and I also try to take care of my surroundings and also watch their movements, hence they don’t need any vaccination.”
Haruna’s response captures the perception of several households in Kano State where there remains a lack of public trust in the effectiveness of vaccination campaigns aimed at reducing the spread of disease during epidemics.
Known as vaccine hesitancy, the reluctance of some individuals within the population to receive safe and recommended available vaccines is mostly driven by a general distrust in the government and health institutions in charge of vaccination and a history of unethical medical trials.
For Kano, SOLACEBASE recalled that the history of vaccine hesitancy goes back to year 2000 when Pfizer, a U.S. pharmaceutical company, launched a new antibiotic drug, Trovan. Nigeria experienced one of the worst meningitis epidemics in its history in 1996, with 109,580 cases and 11,717 deaths.
Read Also: Lawyer arraigned for forging client’s signature
After learning of the meningitis epidemic, Pfizer decided to use it as an opportunity to test the efficacy of Trovan in pediatric settings. It set up a site in the state and selected a sample of 200 children between 3 months and 18 years old to participate over two weeks.
One month later, 11 of the children that had participated died. Additionally, several parents of children involved in the trials reported disabilities among their children, including paralysis and liver failure.
In December 2000, The Washington Post published investigations, accusing Pfizer of conducting unethical experimental trials without attaining informed consent from the participants. Residents say it is an experience they will not forget in a hurry. Almost 27 years later, they remain sceptical about vaccines.
Read Also: Solacebase trains journalists on investigative health reportage at grass-root
Kauranmata said that the state government worked with traditional and religious leaders to deal with the challenge of vaccine hesitancy. For the hard-to-reach areas, he said that the government deployed an outreach team and used local vigilantes who provided security.
Way out?
The World Health Organisation reports that Diphtheria cases and outbreaks can only be prevented by attaining high coverage with 3 doses of a diphtheria-containing vaccine and recommended booster doses.
A medical consultant, Dr Patricia Akintan, involved in case management at LUTH advised that booster doses should be administered between ages 4-7, then at age 10, and subsequently every 10 years.
Apart from making concerted efforts to increase vaccination coverage, researchers argued that the government must also improve access to healthcare facilities, strengthen surveillance systems, raise community awareness, and improve access to clean water and proper sanitation practices.
Adetifa adds that Individuals with signs and symptoms suggestive of diphtheria should isolate themselves and notify their state disease surveillance officer, their State Ministry of Health helpline, or the NCDC through our toll-free line on 6232.
In an interview with SOLACEBASE, Public Health Management Specialist, Dr Laz Ude said that states must as a matter of urgency, enact funds and implement policies on health securities and ensure that all children are fully immunised.
Read Also: PHOTOS: Dilapidated PHC in Jigawa community, residents cry for help
“They should ensure every community has a standing health committee coordinating health promotion activities.”
He also said that effective environmental sanitation and food hygiene measures should be implemented in a sustainable manner and potable water made available and accessible to all residents.
Kauranmata said that the current administration must do well to provide more manpower that will man the facilities to ensure surveillance against the disease and also provide more finance for new innovations that will reposition the healthcare system and sustain the gains already achieved.
This SOLACEBASE publication is produced with support from the Wole Soyinka Centre for Investigative Journalism (WSCIJ) under the collaborative Media Engagement for Development, Inclusion and Accountability project (CMEDIA) funded by the MacArthur Foundation.

Comments are closed.